Inner ligament tear of the knee joint
Acute care & follow-up treatment
ÜBERSICHT
Around 40% of all ligament injuries to the knee joint involve an injury to the medial colleteral ligament (MCL). The most common cause of injury to the medial ligament is sports injuries. If the knee joint is pushed into an increased X-leg position by a direct trauma, this results in an injury to the medial collateral ligament complex. Depending on the extent of the force exerted on the knee joint, the ligament may be overstretched, torn or completely torn off. I also frequently see a torn medial collateral ligament in severe rotational injuries in combination with cruciate ligament tears. As parts of the medial ligament are firmly attached to the base of the medial meniscus, meniscus injuries also occur more frequently.
Structure of the inner ligament
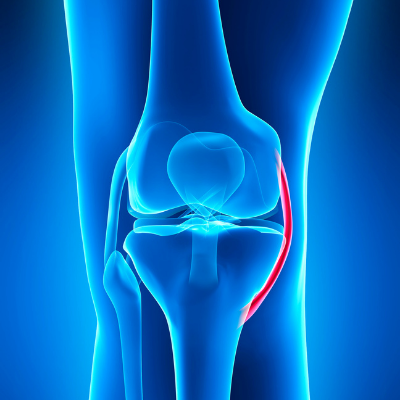
The inner and outer collateral ligament complexes stabilize the knee joint against lateral movements. The medial collateral ligament has an average length of 7-9 cm and is connected to the base of the medial meniscus. Due to this rigid situation, it is much more prone to injury than the collateral ligament. This is an independent ligament that runs from the thigh to the head of the fibula. In the complex anatomy of the knee joint, there are dynamic stabilizers (tendon attachments of the muscle groups) in addition to the rigid stabilizers.
Clinic of a torn medial collateral ligament
In most cases, a suspected medial collateral ligament injury can already be suspected from the medical history. Direct pressure pain is often found at the origin of the ligament, on the inside of the thigh. There is often local swelling, but also a knee joint effusion (e.g. in the case of combined injuries with a cruciate ligament rupture).
The most important diagnostic tool is the clinical examination. Here, the stability of the medial ligament complex can be directly assessed, always in direct comparison with the healthy opposite side, when the joint is opened up. Depending on the extent of the increased opening of the ligament, a distinction can be made between an overstretching, a partial tear or a complete tear of the ligament(grades I-III).
An MRI examination can best visualize the ligament and should definitely be carried out if there is increased clinical opening.
Treatment of torn medial knee ligaments
- Grade I (overextension) and grade II (partial tear) injuries are mainly treated conservatively. Depending on the extent of the pain and the degree of injury, short-term stabilization with a knee joint orthosis can alleviate the acute symptoms. First and foremost, decongestant measures should be taken and physiotherapy started at an early stage. The aim of this is to achieve good mobility as quickly as possible and avoid muscle breakdown.
- Grade III (complete tearing of the ligament) injuries also show comparable results with conservative therapy as with surgical therapy. In this case, a knee joint orthosis is worn for 6 weeks and the range of motion is gradually increased every 2 weeks.
When is surgery performed on a torn medial knee ligament?
Surgery is only necessary in exceptional cases:
- High functional requirements
- with additional concomitant injuries such as multiple ligament tears
- Parts of the ligament impacted into the joint
