Anatomy of the knee joint
An explanation
ÜBERSICHT
The knee joint is the largest joint in the human body. This is where the thigh bone (femur), the shin bone (tibia) and the kneecap (patella) join together. This structure allows us to flex up to 140° and sometimes, especially in women, a slight hyperextension of 5°. The kneecap glides over the thigh bone in a sliding groove which protects it from jumping out to the side. When taking a step, five times the body weight is sometimes placed on the joint.
Joint capsule
The entire joint is enclosed by a large joint capsule. This is lined on the inside with a mucous membrane that produces synovial fluid. This fluid nourishes the joint cartilage and reduces the frictional forces of the individual joint partners. In the event of meniscus damage, cartilage injuries or other irritation in the joint, more fluid is produced. The increasing pressure can cause the fluid to leak backwards at a weak point in the joint capsule, resulting in the formation of a so-called Baker’s cyst. The fluid can reabsorb itself when the irritation is eliminated. The Baker’s cyst is therefore only a symptom of another underlying problem.
Cartilage
The surfaces of the joint partners are covered with a smooth hyaline cartilage layer, which enables friction-free movement. It acts as a shock absorber and protective layer for the bone. As the cartilage has no blood supply of its own, no primary healing can take place. Furthermore, cartilage is not supplied by nerves, which is why cartilage damage alone is not painful. Pain only occurs when the mucous membrane of the joint capsule, which surrounds the entire joint, is irritated by cartilage damage or the bone is exposed.
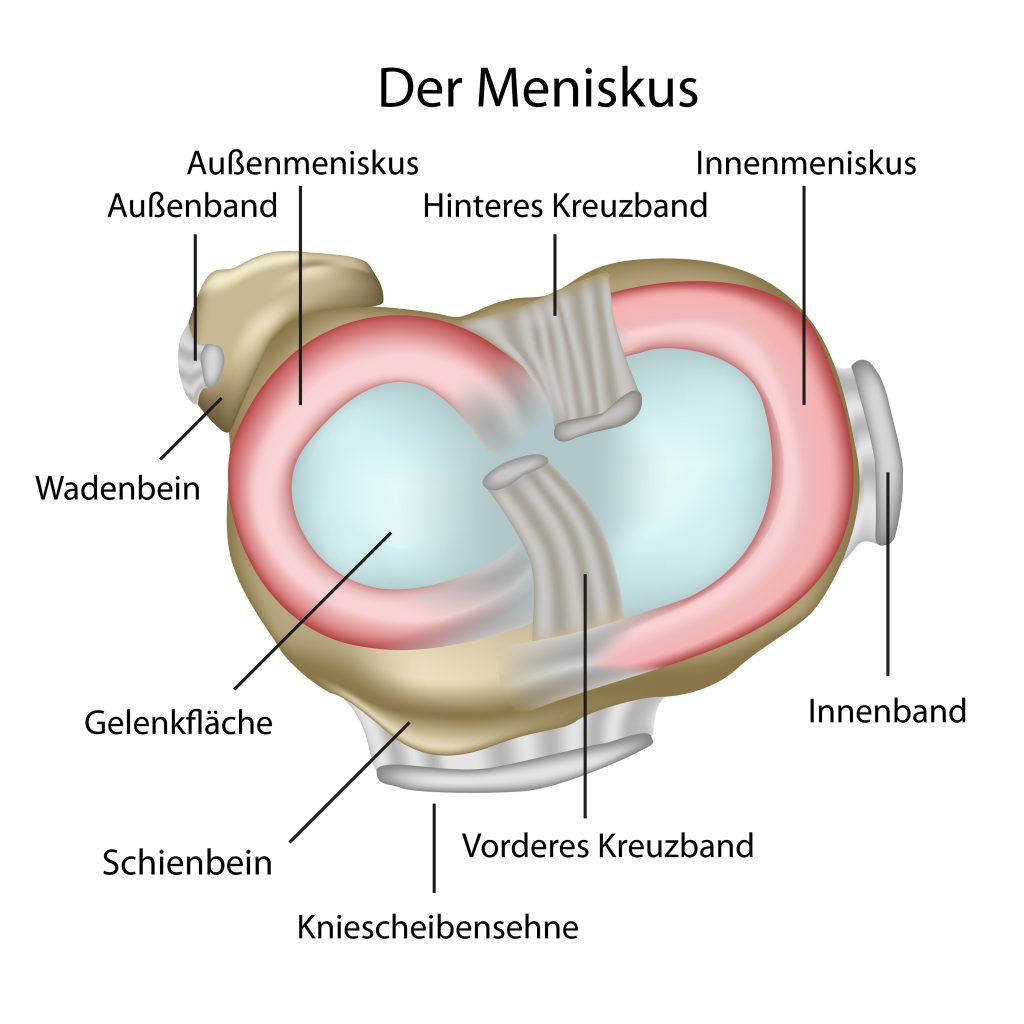
Meniscus
Two menisci lie between the cartilage layer of the thigh and lower leg and act as shock absorbers as they increase the surface area of the joint. They have a crescent shape and can therefore ideally distribute the load of the body weight in all degrees of flexion. The outer meniscus (lateral meniscus) can move forwards and backwards by up to 2 cm between extension and flexion. The medial meniscus is less flexible as it is firmly attached to the joint capsule. This also makes it more susceptible to injury in the event of trauma. After complete removal of a meniscus, the pressure peaks on the cartilage can increase 200-fold, which means that premature wear and tear of the joint is inevitable.
The meniscus is divided into three zones due to its reduced blood supply and therefore also reduced healing potential. The “red zone” near the base is supplied by tiny blood vessels, which is why scarring is possible here after a meniscus suture. The last extensions of blood vessels can also be found in the middle “red-white” zone . A meniscus suture is also conceivable here. In the innermost “white zone” close to the joint, there is no longer any blood supply, which is why healing is no longer possible here. Among specialists , the credo “Save the meniscus!” prevails in order to prevent the early development of osteoarthritis.

Tapes
A complex interplay between bones, ligament complexes, muscle attachments and tendons stabilize the joint even under maximum load, e.g. during sport. In simple terms, there are 4 main ligaments that protect the knee against rotation and axial tilt.
The anterior cruciate ligament and posterior cruciate ligament are located centrally in the joint and stabilize it in all degrees of flexion against rotational movements on the one hand and against forward and backward movements on the other. Both ligaments consist of two main bundles that are twisted against each other. The cruciate ligaments are taut at all times, regardless of whether the knee is extended or flexed. The anterior cruciate ligament stops the lower leg from sliding forwards, while the posterior cruciate ligament prevents it from sliding backwards.
The inner and outer collateral ligament complexes stabilize the knee joint against lateral movements. The medial collateral ligament has an average length of 7-9 cm and is connected to the base of the medial meniscus. Due to this rigid situation, it is much more prone to injury than the collateral ligament. This is an independent ligament that runs from the thigh to the head of the fibula.
Injuries to one or more of these ligaments result in mild to severe instability, which can cause cartilage and meniscus damage over time, depending on the demands placed on the joint. Due to the poor healing potential of both structures, irreversible wear and tear occurs over time, which can lead to full-blown osteoarthritis.
Kneecap
The kneecap (patella) is the largest sesamoid bone in the human body and is embedded in the quadriceps tendon (thigh extensor). By extending the lever arm, it multiplies the force development of the quadriceps. And distributes the enormous forces over the joint surface. Its underside is completely covered with a thick layer of cartilage. In flexion and extension, the kneecap covers a distance of approx. 8-10 cm and slides into the trochlea of the thigh from a knee flexion angle of 30°.
Due to the high forces acting on the kneecap joint (patellofemoral joint), it is particularly frequently affected by osteoarthritis.
Tendons of the knee joint
Of course, the knee joint is far more complicated than just ligaments, bones and meniscus. These are the static stabilizers of the joint. The tendons and muscles surrounding the joint are the dynamic stabilizers. Their role is often underestimated, but they are responsible for many types of knee pain, injuries and, above all, overuse syndromes.
The four-headed quadriceps with the quadriceps tendon and the patellar tendon, which runs from the kneecap to the lower leg, is the strongest extensor of the knee joint. Patellar tendinopathy, degeneration or tears of the quadriceps tendon and patellar tendon tears are just some of the typical injury patterns in this region.
The muscles responsible for knee flexion consist of the biceps femoris (two-headed flexor muscle that attaches to the head of the fibula) and the hamstring muscles (semimembranosus, semitendinosus, gracilis). Part of the hamstring musculature attaches to the inside of the lower leg just below the joint space. A bursa is located here to reduce the frictional forces and is repeatedly responsible for irritation during sporting overload. On the outside, there is a long fascia plate (tractus iliotibialis) which also attaches just below the joint. Runners in particular regularly experience pain here too, which is why irritation in this area is known as runner’s knee .
The calf muscles (gastrocnemius medialis and lateralis) originate at the back of the thigh and extend with the well-known Achilles tendon to the heel bone.
Typical injuries of the knee joint:
Sports involving rapid changes of direction and contact with the body in particular pose a greater risk to the knee joint.
Especially a rupture of the anterior cruciate ligament is a relatively common sports injury. Due to the poor blood supply to the ligament and the immediate instability caused by the tear, the anterior cruciate ligament usually no longer heals functionally in its original position. In the case of untreated injuries to this ligament, the anterior cruciate ligament can scar together with the posterior cruciate ligament. Insufficient function of the cruciate ligament remains and is referred to as Lambda-Wittek healing. An anterior cruciate ligament tear rarely occurs singularly and is therefore often accompanied by meniscus tears, cartilage injuries or other ligament injuries.
A meniscus tear usually occur during rotational movements with the lower leg in a fixed position (football, skiing, etc.) or due to chronic overloading in occupations involving the knee. As a concomitant injury of the anterior cruciate ligament rupture, it increasingly destabilizes the joint. A torn meniscus can protrude into the joint and cause a functional restriction of mobility. This must be examined immediately by a specialist, otherwise the meniscus and cartilage tissue will be destroyed.
Also Dislocations of the kneecap (patellar luxation) also occur regularly if there has been direct trauma to the inside of the kneecap or if there is a predisposition to it due to a congenital malformation of the kneecap stabilizers.
The internal ligament tear is certainly one of the most common ligament injuries to the knee joint. Fortunately, minor injuries to the medial collateral ligament heal conservatively and largely without consequences. In the case of more severe injuries, it is not uncommon for residual instability to remain, which is why an inner ligament injury should always be assessed by a sports orthopaedist.
Athletes have ever-increasing demands on their joints and naturally want to return to their usual sport under competitive conditions as quickly as possible. Sports orthopaedists therefore often have to strike a balance between getting the patient fit again as quickly as possible and ensuring that the injury has healed well enough to withstand the strain. Consequential injuries should also not occur, which is why close cooperation with physiotherapists is essential.