Cruciate ligament surgery in Vienna
Cruciate ligament surgery
Modern cruciate ligament surgery for maximum stability
A torn ACL is one of the most common sports injuries – especially in sports such as soccer, handball, tennis or skiing. While a partial tear can sometimes be treated conservatively, a complete tear of the anterior cruciate ligament often leads to persistent instability of the knee. For those affected, this means: uncertainty in everyday life, pain during exercise and an increased risk of consequential damage to the meniscus or cartilage.
Cruciate ligament surgery (cruciate ligament plastic surgery) is the most effective method of restoring long-term stability to the knee and enabling a safe return to sport and everyday life.
OVERVIEW
When is cruciate ligament surgery advisable?
Not every cruciate ligament rupture automatically requires surgery. However, there are clear situations in which surgery is the better choice:
- Complete cruciate ligament rupture: The anterior cruciate ligament does not grow back together on its own.
- Instability in everyday life: the knee "buckles" (so-called giving way attacks).
- High athletic stress: Especially in sports with many changes of direction or jumps (e.g. soccer, handball, skiing).
- Young, active patients: to prevent secondary damage and premature joint wear.
- Concomitant injuries: such as meniscus or cartilage damage, which can be treated in the same operation.
Advantages of modern cruciate ligament surgery
- Arthroscopic technique: small incisions, earlier rehabilitation possible
- High success rate: restoration of stability in over 90% of patients
- Treatment of concomitant injuries possible in the same operation
- Individual choice of graft depending on the patient and sporting activity
- Short inpatient stay: often only one overnight stay in hospital necessary
For older patients or people who do not engage in intensive sport, conservative therapy may be sufficient under certain circumstances.
Conservative treatment of a cruciate ligament rupture
Just because no surgery is performed does not mean that no therapy is necessary. Targeted measures are also crucial in conservative treatment in order to maintain the function and stability of the knee.
Immediately after the injury, the focus is on pain relief and reducing swelling – through cooling, elevation and compression. Physiotherapy should then be started as soon as possible to restore the joint’s mobility.
Particular attention is paid to strengthening the knee flexor muscles (hamstrings). These muscles pull the lower leg backwards, thereby protecting the cruciate ligament and stabilizing the injured ligament. Proprioceptive exercises are also important: balance and coordination training trains depth sensitivity, which also improves the stability of the knee joint.
The stability of the knee should be checked regularly in the further course of treatment. If the joint remains unstable despite conservative treatment or if “giving way” attacks occur repeatedly, the indication for surgery must be reassessed.
If the knee remains unstable despite intensive conservative therapy or if there are high sporting demands, surgical treatment is often the best solution – there are various surgical methods to choose from.
Choosing the right surgical method
Two modern surgical methods are available in my practice, which are used individually depending on the injury pattern and patient:
Surgical cruciate ligament refixation (cruciate ligament suture)
This method is possible if the cruciate ligament is torn close to the bone and can still be refixed. The ligament is reattached to the bone arthroscopically using special suture anchors. Advantage: preservation of the body’s own cruciate ligament and, in some cases, faster rehabilitation.
Surgical cruciate ligament replacement surgery / cruciate ligament replacement
If the cruciate ligament is severely damaged or completely torn, it is replaced with an autologous tendon graft (e.g. semitendinosus or quadriceps tendon). This technique has been tried and tested for many years and is considered the standard for reliably restoring the stability of the knee in the long term.
Which method is the better choice in each individual case depends on the tear pattern, age, sporting demands and accompanying injuries. In a personal consultation, we will clarify together which operation offers the best solution for you.
Replacement of the cruciate ligament - cruciate ligament replacement surgery
What is cruciate ligament replacement surgery?
The cruciate ligament is a complex interplay of bones, ligament complexes, muscle attachments and tendons. The knee joint can thus be stabilized even under maximum load, e.g. during sport. A simplified distinction is made between 4 main ligaments which protect the knee against rotation and axial tilt.
The most important ligaments in the knee are the anterior and posterior cruciate ligaments, which cross inside the joint and are responsible for stabilizing and controlling forward and backward movements.

Which tendon for cruciate ligament replacement surgery?
Hamstring tendons
Hamstring tendons (semitendinosus and gracilis tendons STG): This is the standard tendon used by many sports orthopaedic surgeons to reconstruct a torn cruciate ligament. The tendon is removed through a 2-3 cm incision on the inside of the tibial plateau or just above the popliteal fossa (post-medial removal), folded several times and reinforced with a special suture construct.
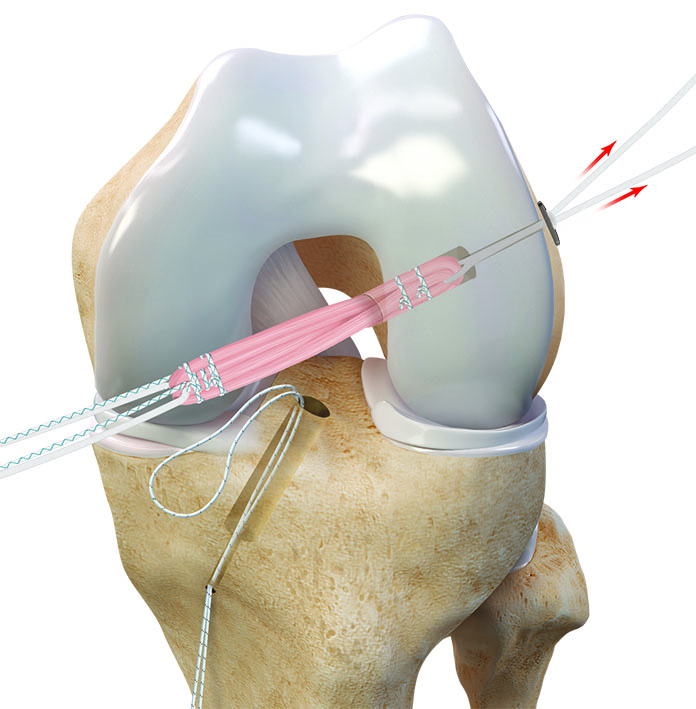
The “all-inside” technique is one of the gentlest methods for cruciate ligament ruptures. The new cruciate ligament is pulled into short, pre-drilled channels using two metal plates in a pulley technique and fixed to the bone. Compared to conventional techniques, which often require two tendons, the semitendinosus tendon is sufficient here – the second hamstring tendon remains untouched.
The tendon is removed through a 2-3 cm long skin incision just above the popliteal fossa (post-medial tendon removal). This spares a cutaneous nerve (infrapatellar ramus), which is damaged in up to 10 % of cases with conventional methods, which can lead to loss of sensitivity on the inside of the lower leg.
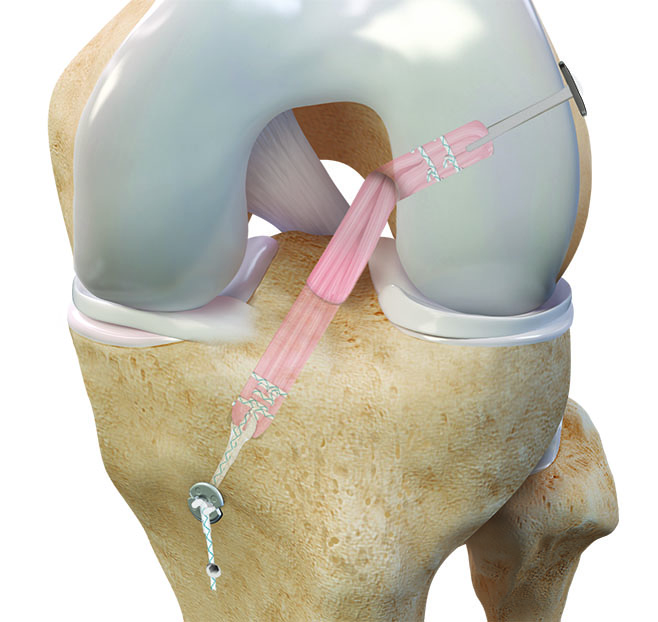
The graft is prepared with two adjustable suture loops (Tightrope) and metal plates and moistened in an antibiotic solution to reduce the risk of infection to almost zero. Two bone channels are then created in the thigh and tibial plateau (at the anatomical origin of the cruciate ligament). Once the transplant has been inserted, the metal plates “flip” on the outside of the bone and fix the ligament securely in place.
Advantages of this technique: anatomical positioning, particularly strong primary fixation, individually strong graft can be selected
Patellar tendon
Patellar tendon (=patellar tendon) BTB ( =bone tendon bone): In a patellar tendon graft, the middle third of the tendon is harvested with a bone block from the kneecap and another bone block from the tibial plateau.
One advantage is the faster return to sport compared to other grafts, as the bone blocks grow into the bone canals faster than other cruciate ligament grafts.
Quadriceps tendon
Quadriceps tendon: The middle superficial third of the quadriceps tendon is harvested through an approx. 3-4 cm long incision just above the kneecap.
One advantage is that the graft can be harvested either with a bone block from the kneecap or without.
For minimally invasive quadriceps tendon harvesting, an approx. 3-4 cm skin incision running vertically from the kneecap upwards is usually sufficient. Thanks to the special harvesting tool, a graft of varying thickness can be selected depending on body and bone size. Once part of the tendon has been removed, the resulting gap is closed. I also use a special suture loop for the quadriceps tendon, which is firmly sutured to the tendon. A small metal plate is attached to the adjustable suture loop (tightrope), against which the tendon can be firmly tightened using
Allograft
Allograft (donor tendon from a cadaveric donation): Thanks to newer methods of processing cadaveric tendons, there are hardly any disadvantages today compared to the body’s own tendons.
Your cruciate ligament specialist
Find out more about cruciate ligament surgery & treatment for a torn cruciate ligament in this video!
How is a cruciate ligament rupture operated on?
Nowadays, an individualized treatment approach is in keeping with the times. For me, it is no longer enough to use the same cruciate ligament transplant for every patient. Different bone sizes, leg axes, concomitant injuries or favored sports (jumping or sprinting) all play a part in the individual treatment algorithm.
In many cases, the anterior cruciate ligament does not tear singularly. Concomitant injuries such as meniscus tears, capsules or ligament injuries are common. Therefore, the timing of the operation should be considered, as well as any additional interventions to increase the stability of the joint.
During a diagnostic arthroscopy (= keyhole technique), the entire joint is inspected from the inside with a camera through skin incisions measuring just 2×0.5 cm. This means that injuries to the cartilage surface and meniscus tears can also be treated.

Rehabilitation after cruciate ligament surgery
After arthoroscopic cruciate ligament surgery, patients can usually leave the hospital on the second day after the operation. Physiotherapeutic treatment takes place during the inpatient stay, but must be continued immediately afterwards in order to regain full freedom of movement as soon as possible.
A splint is not usually necessary. For accompanying meniscus sutures or cartilage surgery, immobilization with a motion orthosis and partial weight bearing with crutches is necessary during the first 6 weeks.
After a cruciate ligament injury, there is a higher risk of re-injury to the same knee, but also to the other knee. A cruciate ligament prevention program is therefore essential for further sporting activities.
Frequently asked questions - FAQ cruciate ligament surgery
How does cruciate ligament surgery work?
Today, cruciate ligament surgery is almost always performed minimally invasively (arthroscopically). This means smaller incisions, less pain and faster healing.
Step 1 – Preparation
After diagnosis by clinical tests and MRI, a decision is made as to which surgical technique is most suitable. The cruciate ligament is often replaced with the body’s own tendons (tendon graft).
Step 2 – Selecting the graft
Patellar tendon
Hamstring tendon
Quadriceps tendon
Allograft
Step 3 – Operation
The torn cruciate ligament is removed.
The tendon graft is placed in the exact position of the original cruciate ligament.
is fixed in place with special screws or implants.
The operation usually takes 40–60 minutes and is performed under general or spinal anaesthesia.
Can a torn cruciate ligament also be stitched?
Good long-term results can be observed with cruciate ligaments that have been torn directly from the bone. Tears in the middle of the ligament should rather be treated with a replacement plastic.
The timing is crucial! Only injuries that are reattached to the bone in the first 3 weeks are likely to be successful. It is also known that the probability of a cruciate ligament suture failing again is higher than a cruciate ligament plastic surgery tearing again. It is therefore advisable to refrain from cruciate ligament sutures in young athletes.
When is cruciate ligament suturing possible?
Patient age (>25)
Surgery within 3 weeks
Cruciate ligament torn off directly at the bone
How long does it take to heal after cruciate ligament surgery?
A cruciate ligament that has been operated on must first heal back into the bone before it can provide good long-term stability. This takes several months.
Milestones in rehabilitation:
(1) Full load within the first 2 weeks
(2) The patient is usually fit for work after 6-8 weeks
(3) Cycling is permitted after approx. 6-8 weeks
(4) Running only after 3 months
(5) It is possible to return to your usual sport after 6 months
(6) Fit for competition after 9-12 months at the earliest
How long do you need crutches after cruciate ligament surgery?
After a simple cruciate ligament replacement, you only need crutches for 2 weeks. If the meniscus has also been sutured, you usually have to use crutches for 6 weeks.
How soon after a cruciate ligament rupture does surgery need to be performed?
The operation should be performed eitherin the first 10 days or after the primary irritationhas subsided(approx. 6 weeks). If surgery is performed during the irritation phase, the likelihood of severe scarring of the entire joint (=arthrofibrosis) increases.
Does a cruciate ligament rupture always require surgery?
Cruciate ligament ruptures do not always have to be operated on immediately! If the joint is unstable after a cruciate ligament rupture , surgery should be performed. If you are young and active in sports, surgery should be favored in order to avoid permanent damage. If the requirements are low, the patient is older and has little sporting ambition, and there is no tangible instability, conservative treatment can be chosen without any problems.
Can a cruciate ligament rupture heal without surgery?
The function of the cruciate ligament can sometimes be well compensated for by a strong muscle sheath. As the cruciate ligament lies in the middle of the joint and the joint is filled with synovial fluid, no haematoma can form, which is so important for healing. In individual cases, scarring can occur with the posterior cruciate ligament. However, functional healing of the anterior cruciate ligament after a complete tear is very unlikely.
How long in hospital after cruciate ligament surgery?
You should expect to stay in hospital for 1-2 days after a cruciate ligament reconstruction.
When can I drive again after cruciate ligament surgery?
This mainly depends on which leg was operated on. If the left knee was operated on and you drive a car with automatic transmission, you can often drive after 3-4 weeks. However, if the right knee has been operated on, it usually takes 6 weeks or longer, as the joint must be stable enough to be able to brake quickly and powerfully in an emergency. It is important that patients only drive again when they can react safely and without restriction. The treating doctor should always be consulted before resuming driving.
When can I return to work after cruciate ligament surgery?
This depends very much on the type of activity:
Office work or sedentary activities: usually possible again after 2-3 weeks.
Physically demanding occupations (e.g. construction workers, care workers): often only realistic after 3-4 months.
It is crucial that the knee is sufficiently resilient and stable. The return to work is individually coordinated with the doctor.
How high is the risk of the cruciate ligament tearing again?
Depending on the study, the risk of a new cruciate ligament rupture is around 5-10%. The first 2 years after the operation are particularly at risk, as the transplant still has to heal and adapt to the strain. The other, healthy cruciate ligament can also have an increased risk of injury if the knee is not sufficiently stabilized or the muscles are not trained well enough. This risk can be significantly reduced through consistent rehabilitation, targeted muscle training, proprioceptive training and a gradual return to sport.
Which anesthesia is used for cruciate ligament surgery?
Cruciate ligament surgery is performed either under general anesthesia or spinal anesthesia (anesthesia from the hip downwards). Which method is chosen depends on the individual requirements and wishes of the patient. Both methods are safe and enable pain-free surgery.
What role does physiotherapy play after cruciate ligament surgery?
Physiotherapy is an indispensable part of follow-up treatment. It often begins just a few days after the operation and accompanies the patient for many months.
The goals are:
– Reduce swelling and restore mobility
– Muscle development of the thigh and core muscles
– Stabilization and coordination training to make the knee safe in all everyday situations
– Gradual load build-up through to sport-specific training
Without physiotherapy, there is a high risk that the knee will remain permanently unstable, the muscles will break down or movement will be restricted.
What happens if you don't operate on a torn cruciate ligament?
An untreated cruciate ligament rupture can lead to permanent instability. As a result, meniscus damage, cartilage injuries and premature osteoarthritis are common. Although some patients can compensate for the missing ligament for a while with a strong muscle sheath, there is a risk of serious consequential damage in the long term. This is why medical assessment and treatment planning are crucial.
What are the risks of cruciate ligament surgery?
Cruciate ligament surgery is a proven and safe procedure, but – as with any operation – there are certain risks. The general surgical risks include infections, wound healing disorders and thrombosis. Particularly after cruciate ligament surgery, arthrofibrosis (scarring in the joint), restricted movement or, in rare cases, loosening or re-tearing of the graft can also occur. However, these risks can be greatly reduced through modern, minimally invasive surgical techniques, sterile conditions, consistent physiotherapy and close follow-up care. It is important that the patient and doctor work together to ensure consistent aftercare.
Can a cruciate ligament rupture be prevented?
A cruciate ligament rupture cannot be 100% prevented, but the risk can be significantly reduced. Important measures include
– Targeted strength training, especially of the thigh and core muscles
– Proprioceptive training (balance exercises, jumping and landing techniques)
– Sport-specific technique training (e.g. correct braking and landing in soccer or handball)
– When skiing: correctly adjusted bindings and good skiing technique
What are the chances of success for cruciate ligament rupture surgery?
Most patients achieve lasting stability after cruciate ligament surgery and can return to everyday life and sport. Studies show success rates of over 90 % if the operation is combined with consistent rehabilitation. The surgeon’s experience, the correct surgical method and the patient’s active cooperation in the follow-up treatment are crucial.
Do you have further questions or would you like to have your personal situation clarified by an orthopaedic specialist?
I, Dr. Gustav Timmel, cruciate ligament specialist from 1030 Vienna, take the time for a detailed examination and advise you individually on the best treatment options – from the initial consultation and diagnosis to conservative therapy and surgery.
Make an appointment now at my practice in Vienna – together we will find the best way back to stability, safety and freedom of movement.

{kind=link}
{kind=link}
{kind=link}